What is COPD?
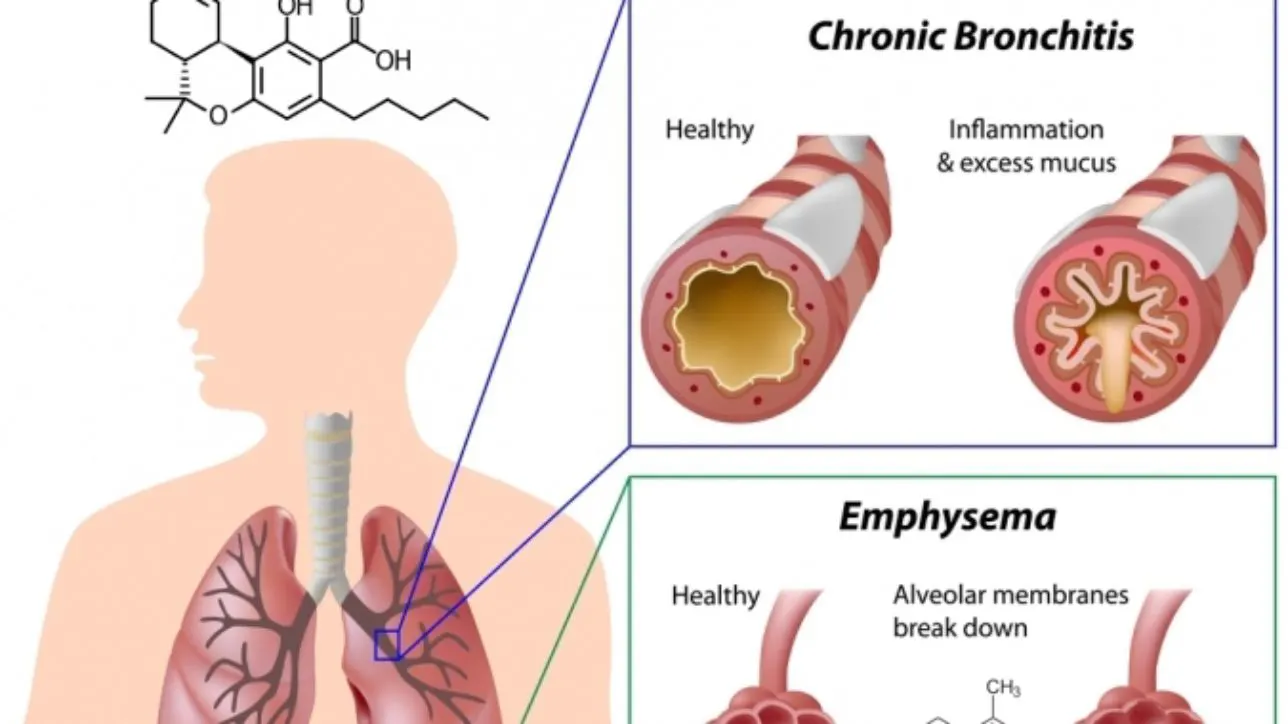
Chronic obstructive pulmonary disease (COPD) is an illness characterized by increased production of mucus and chronic inflammation of the airways resulting in reduced respiratory capacity. The two primary forms of COPD are chronic bronchitis, which produces a long-term cough with mucus, and emphysema, which leads to the progressive deterioration of the alveoli, the air sacs that allow for gaseous exchange in the lungs.
How is COPD treated?
COPD is typically treated with two different types of compounds: beta-adrenergic agonists and corticosteroids. Beta-adrenergic agonists are bronchodilators, which relax the smooth muscle surrounding the respiratory tract resulting in an increased diameter of the bronchial passages facilitating airflow. There are two types of beta-agonists: short-acting beta-adrenergic agonists (SABAs) such as albuterol and long-acting beta-adrenergic agonists (LABAs) such as salmeterol. SABAs are typically utilized in the event of an acute attack of shortness of breath while LABAs are used as a prophylactic measure. LABAs are commonly co-administered with corticosteroids such as fluticasone, which acts as a preventative against immune-mediated inflammation of the airways. One such formulation of LABAs and corticosteroids is the drug Advair, a combination of salmeterol and fluticasone.
How might cannabis help patients with COPD?
All smoke irritates the lung and aggravates COPD, but vaporized or ingested cannabis could potentially provide many benefits.
1. Bronchodilatory effects
Studies performed in the 1970’s at the University of California Los Angeles by Donald Tashkin have shown that both inhaled and orally ingested THC produce bronchodilation for up to two hours after administration [1]. Further investigations by the Respiratory Pharmacology Laboratory in Paris have shown that CB1 receptor activation inhibits cholinergic contraction in a concentration-dependent fashion, offering a possible mechanism for acute bronchodilation associated with cannabis intake [2]. Although smoked cannabis also has this effect, any kind of combustion creates other lung irritants that would be counterproductive for COPD treatment.
2. Suppression of the immune system
Those with COPD have a heightened immune response in the lungs and compounds in cannabis can lead to immunosuppression. Studies have shown that THC induces rapid mobilization of a specific subset of white blood cells that arise from bone marrow called myeloid-derived suppressor cells (MDSCs)[3]. These cells exert potent immunosuppressant properties by inhibiting the proliferation and activation of T-cells.
Additional studies performed at the University of South Carolina School of Medicine support these findings, where they determined that the intraperitoneal (injection into the body cavity) application of THC causes changes in microRNA expression that promotes the suppression of the immune system [4]. Other findings using murine models have shown that intraperitoneal administration of THC results in a reduction of allergen-induced mucus production [5].
3. Anti-inflammatory effects
Cannabinoids have anti-inflammatory benefits through a variety of mechanisms. The acidic cannabinoids have a greater anti-inflammatory capacity than their non-acidic counterparts. Specifically studies by Ruhaak, et al., have shown that cannabinoids, in particular the acidic cannabinoids, are capable of inhibiting cyclooxygenases (COX-1 and COX-2); which are the enzymes responsible for the production of inflammatory compounds such as prostaglandins and thrombaxanes. Their investigation found that cannabigerolic acid (CBGA) was the most potent inhibitor of all the cannabinoids tested having an IC50 value of 4.6 x 10-4 M and 2.0 x 10-4 M for COX-1 and COX-2 respectively [6].
Recently studies performed at the University of Sao Paulo using cannabidiol have also shown some potential for improving the symptoms of COPD. They found decreased pulmonary inflammation and improvements in lung function in murine models of inflammatory lung disease using the inflammatory agent LPS, a component of the cell wall in gram-negative bacteria, as the inflammatory agent [7].
Other studies of terpene compounds, the aromatic components found in cannabis show anti-inflammatory benefits as well. In particular, beta caryophyllene has been shown to act as a dietary cannabinoid, attenuating inflammatory responses in various tissues in a CB2 receptor-dependent fashion [8-10]. In addition to being found in cannabis this terpene is also found in high concentrations in black pepper and cloves.
Conclusion
These studies indicate that cannabis could potentially act as a means to mitigate acute attacks of bronchoconstriction and may also act as a prophylactic measure for patients with COPD. However, human trials are needed to confirm some of these benefits and until restrictions by the federal government are lifted, a deeper understanding of these mechanisms will remain poorly understood.
References
1. Tashkin DP, Shapiro BJ, Frank IM. Acute effects of smoked marijuana and oral delta9-tetrahydrocannabinol on specific airway conductance in asthmatic subjects. Am Rev Respir Dis. 1974;109(4):420-8.
2. Grassin-delyle S, Naline E, Buenestado A, et al. Cannabinoids inhibit cholinergic contraction in human airways through prejunctional CB1 receptors. Br J Pharmacol. 2014;171(11):2767-77.
3. Hegde VL, Nagarkatti M, Nagarkatti PS. Cannabinoid receptor activation leads to massive mobilization of myeloid-derived suppressor cells with potent immunosuppressive properties. Eur J Immunol. 2010;40(12):3358-71.
4. Hegde VL, Tomar S, Jackson A, et al. Distinct microRNA expression profile and targeted biological pathways in functional myeloid-derived suppressor cells induced by Δ9-tetrahydrocannabinol in vivo: regulation of CCAAT/enhancer-binding protein α by microRNA-690. J Biol Chem. 2013;288(52):36810-26.
5. Reddy AT, Lakshmi SP, Reddy RC. Murine model of allergen induced asthma. J Vis Exp. 2012;(63):e3771.
6. Ruhaak LR, Felth J, Karlsson PC, Rafter JJ, Verpoorte R, Bohlin L. Evaluation of the cyclooxygenase inhibiting effects of six major cannabinoids isolated from Cannabis sativa. Biol Pharm Bull. 2011;34(5):774-8.
7. Ribeiro A, Almeida VI, Costola-de-souza C, et al. Cannabidiol improves lung function and inflammation in mice submitted to LPS-induced acute lung injury. Immunopharmacol Immunotoxicol. 2014;:1-7.
8. Bento AF, Marcon R, Dutra RC, et al. β-Caryophyllene inhibits dextran sulfate sodium-induced colitis in mice through CB2 receptor activation and PPARγ pathway. Am J Pathol. 2011;178(3):1153-66.
9. Horváth B, Mukhopadhyay P, Kechrid M, et al. β-Caryophyllene ameliorates cisplatin-induced nephrotoxicity in a cannabinoid 2 receptor-dependent manner. Free Radic Biol Med. 2012;52(8):1325-33.
10. Gertsch J, Leonti M, Raduner S, et al. Beta-caryophyllene is a dietary cannabinoid. Proc Natl Acad Sci USA. 2008;105(26):9099-104.