What are migraines?
Throbbing, pulsating, and excruciatingly painful, migraine headaches can be debilitating and affect over 23 million people in the US alone. Migraine headaches are recurrent headaches that typically affect one side of the head and are often accompanied by nausea. Migraines induce a state of hyperalgesia in a patient causing sensitivity to stimuli that would not normally cause pain. Though some pieces of the puzzle have been assembled, a complete picture of why migraine headaches occur has not yet been fully elucidated. However, what has been determined by researchers is the areas from which this pain arises, some of the molecular changes that occur during a migraine, and how cannabinoids can modify these changes.
What happens during a migraine?
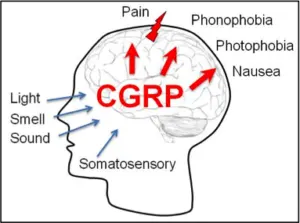
Prior to a migraine attack, levels of the neurotransmitter serotonin are substantially increased and subsequently, during the headache that follows these levels drop to below normal[1]. During a migraine neurons in the trigeminal ganglia also release neuropeptides called Substance P, Neurokinin A, and calcitonin gene-related peptide (CGRP). The release of these neuropeptides leads to vasodilation and an increase in pro-inflammatory molecules in the surrounding area leading to irritation of the nerve and hyperalgesia (increased sensitivity).
How can cannabis prevent migraine headaches?
As previously mentioned, alterations in serotonin levels have been linked to migraines and it has been shown that there is some interplay that occurs between cannabinoids and the serotonergic system. These alterations arise from the release of serotonin from platelets causing a spike of serotonin in the blood. This spiking is the first step in the generation of a migraine. Cannabis can be used as a prophylactic in these scenarios because it has been shown to prevent this release of serotonin from blood platelets [2]. In addition, THC has also been shown to increase serotonin synthesis, which could also help mitigate the deficits from migraine depletion [3].
How does cannabis alleviate migraine symptoms?
Cannabis has long history of use for relief from pain and nausea and our own endocannabinoids also have an influence on these states. This led researchers to believe that migraines could be classified as a clinical endocannbinoid deficiency (CECD). The support for this idea comes from the observation that body’s endogenous cannabinoid anandamide along with other cannabinoid receptor partial agonists, like THC, augment serotonin release and the way the serotonergic system relays pain information [4]. For example, anandamide has been shown to produce an inhibitory effect on a subtype of serotonin receptor called 5-HT3 [5]. This receptor is a mediator of emesis (vomiting) and pain responses, which could partially explain how cannabis can alleviate the pain and nausea associated with migraines.
Cannabinoids also have an effect on the areas that are thought to generate this pain. In the trigeminal nerve, cannabinoids have been shown to quell inflammation and produce analgesia [6]. Further research on this area of the brain using synthetic cannabinoid agonists has shown that CB1 receptor activation actually reduces the amount of pain signals produced from this region [7]. Many studies have also consistently cited an area of the brain called the periaqueductal gray matter (PAG) in the generation of migraines [8]. Studies on this area of the brain using synthetic cannabinoid agonists (compounds similar to THC) have shown reduced responses to pain [9].
Future Research
Researchers have concluded that cannabinoids interact with the serotonergic system and the trigeminal nerve to provide preventative benefits as well as relief from migraine symptoms. Though much progress has been made in understanding the mechanisms of migraines and how cannabinoids augment them, to date there have been little to no human studies performed to fully confirm these findings. However, regardless of a lack of clinical studies there is a mountain of anecdotal evidence and preclinical data to support the use of cannabis for migraine prevention and treatment.
References
- Szczudlik A. The role of serotonin in the pathophysiology of migraine. Neurol Neurochir Pol. 1992;Suppl 2:14-27.
- Volfe Z, Dvilansky A, Nathan I. Cannabinoids block release of serotonin from platelets induced by plasma from migraine patients.Int J Clin Pharmacol Res. 1985;5:243-6.
- Johnson KM, Dewey WL. The effect of delta9-tetrahydrocannabinol on the conversion of [3H]trypotphan to 5-[3H] hydroxytryptamine in the mouse brain. J Pharmacol Exp Ther. 1978 Oct;207:140-50.
- Russo EB. Clinical endocannabinoid deficiency (CECD): Can this concept explain therapeutic benefits of cannabis in migraine, fibromyalgia, irritable bowel syndrome and other treatment-resistant conditions?Neuro Endocrinol Lett.2008;29:192–200.
- Fan P. Cannabinoid agonists inhibit the activation of 5-HT3 receptors in rat nodose ganglion neurons. J Neurophysiol. 1995 Feb;73:907-10.
- Liang YC, Huang CC, Hsu KS. Therapeutic potential of cannabinoids in trigeminal neuralgia. Curr Drug Targets CNS Neurol Disord. 2004 Dec;3:507-14.
- Akerman S, Holland PR, Lasalandra MP, Goadsby PJ. Endocannabinoids in the brainstem modulate dural trigeminovascular nociceptive traffic via CB1 and “triptan” receptors: implications in migraine. J Neurosci. 2013 Sep 11;33:14869-77.
- Goadsby PJ, Gundlach AL. Localization of 3H-dihydroergotamine-binding sites in the cat central nervous system: relevance to migraine. Ann Neurol. 1991 Jan;29:91-
- Lichtman AH, Cook SA, Martin BR. Investigation of brain sites mediating cannabinoid-induced antinociception in rats: evidence supporting periaqueductal gray involvement. J Pharmacol Exp Ther. 1996 Feb;276:585-93.
- Raddant AC, Russo AF. Calcitonin gene-related peptide in migraine: intersection of peripheral inflammation and central modulation. Expert Rev Mol Med. 2011 Nov 29;13:e36.