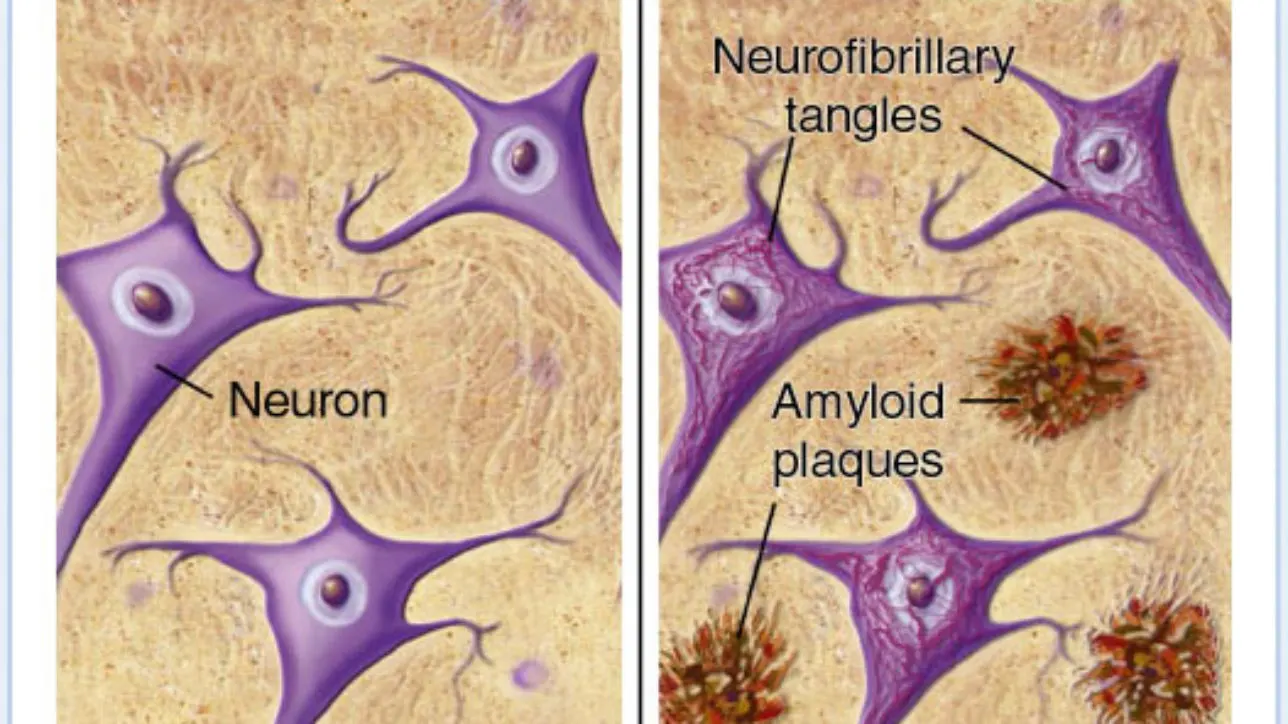
Alzheimer’s Disease (AD) is a neurological disorder that is characterized by a loss of memory and learned behavior. Alzheimer’s normally occurs in adults 65 and older and has no cure. The pathology of the disease includes aggregates of the Aβ protein along with the hyperphosphorylation of tau protein, which ultimately leads to the formation of neurofibrillary tangles. These aggregates and tangles cause excitotoxicity and microglial activation, which prompts inflammatory responses, and ultimately lead to cell death.
Cannabis can inhibit the inflammation caused by the abnormal structures formed by Aβ and tau proteins and can also slow the progression of the disease. Investigators at The Scripps Research Institute in California in 2006 reported that THC inhibits the enzyme responsible for the aggregation of amyloid plaques [acetycholinesterase] — the primary marker for Alzheimer’s disease — in a manner “considerably superior” to approved Alzheimer’s drugs such as donepezil and tacrine. An excerpt from the paper states, “our results provide a mechanism whereby the THC molecule can directly impact Alzheimer’s disease pathology. THC and its analogues may provide an improved therapeutic for Alzheimer’s disease simultaneously treating both the symptoms and the progression of the disease.” (Eubanks, 2006)
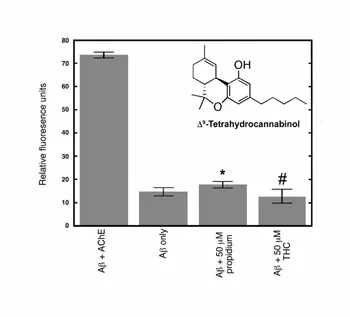
This figure from the Scripps Research Institute study shows THC’s effectiveness in reducing the formation of Aβ plaques by inhibiting the enzyme acetylcholinesterase (AChE).
Synthetic cannabinoids have also shown promise in the treatment of AD. Both in vitro and in vivo studies of WIN-55, 212-2 using Aβ treated cells showed a significant decrease in microglia-mediated neurotoxicity (Ramirez, 2005).
A study published in 2007 by V.A. Campbell thoroughly explains the potential of cannabinoids in AD, “The propensity of cannabinoids to reduce β-amyloid-evoked oxidative stress and neurodegeneration, whilst stimulating neurotrophin expression neurogenesis, are interesting properties that may be beneficial in the treatment of Alzheimer’s disease. Δ9-tetrahydrocannabinol can also inhibit acetylcholinesterase activity and limit amyloidogenesis, which may improve cholinergic transmission and delay disease progression. Targeting cannabinoid receptors on microglia may reduce the neuroinflammation that is a feature of Alzheimer’s disease, without causing psychoactive effects.” (Campbell, 2007)
Newer research has affirmed these positive findings using cannabinoids in mouse models. Researchers from The Roksamp Institute in Sarasota, FL found that the clearance of amyloid beta across the blood brain barrier was doubled in the presence of cannabinoid agonists or inhibitors of the enzymes that degrade cannabinoids (Bachmeier, 2013). This finding is significant because it describes the mechanism of how stimulation of the endocannabinoid system can reduce the burden of Aβ plaques in the brain.
Most recently research published in the journal Neuron from the Stanford School of Medicine has shown that early deficits in Alzheimers such as dementia can be triggered by a loss of the body’s own natural cannabinoids, anandamide and 2-arachidonoylglycerol (2-AG) (Orr, 2014). Based on this research one would think that ingesting exogenous cannabinoids would perform the same role however it would be inaccurate to assume that smoking cannabis could counteract the effects of beta-amyloid plaque on memory and learning “Endocannabinoids in the brain are very transient and act only when important inputs come in,” according to Dr. Daniel Madison, one of the authors of the study. “The primary active ingredient in cannabis, THC, has a much longer lasting effect”.